
Acute cerebellitis
Updates to Article Attributes
Acute cerebellitis (AC), also known as acute cerebellar ataxia, is a rare inflammatory process characterised by a sudden onset of cerebellar dysfunction usually affecting children. It is related as a consequence of a primary or secondary infection, or much less commonly as a result of a post-vaccinal-vaccination reaction.
Terminology
The terms acute cerebellitis and acute cerebellar ataxia are often used interchangeably, as in this article, but they are considered separate by some authors 9. Acute cerebellar ataxia is a milder form of acute cerebellitis or perhaps a mild subset of acute cerebellitis 9.
Epidemiology
Usually occurring in children under six years of age, ACacute cerebellitis is the most common cause of ataxia in the paediatric population. It is reported as a complication of several systemic infectious diseases, such as varicella infection (chickenpox) 6.
Adult cases of cerebellitis are possible and well established in medical literature 5.
Clinical presentation
A broad range of signs and symptoms may be present: fever, tremor, nystagmus, truncal ataxia, dysarthria, headache, nausea, vomiting and consciousness alterations. Signs of meningeal irritation and seizures may be observed less frequently 1,4.
Some relevant complications have been described, such as:
- obstructive hydrocephalus and consequent intracranial hypertension
- tonsillar herniation
- cerebellar trunk compression
- severe cerebellar atrophy 3
Laboratory findings
- CSF pleocytosis 4
Pathology
ACAcute cerebellitis has been associated with a large number of infectious agents, such as: coxsackievirus, echovirus, enteroviruses, Epstein-Barr virus, hepatitis A, herpes simplex virus I, human herpesvirus 6, measles, rubella, mumps, parvovirus B19, Borrelia burgdorferi (Lyme disease), malaria, Mycoplasma pneumoniae, and typhoid fever 2,4,6.
Acute cerebellar ataxia following vaccination for varicella, hepatitis B, and rabies has been reported 6-8.
Radiographic features
CT
Cerebellar images can be normal due the CT limitations on the evaluation of posterior fossa. Nonetheless, complications like compression of the brain stem and obstructive hydrocephalus, when present, are identified on CT images and may guide for further investigation.
MRI
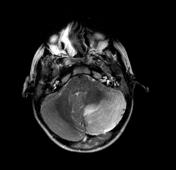
Usually, the cerebellar hemispheres are symmetric. It may show a homogeneous mass effect due the cerebellar swelling 1,4.
- T1: cortical hypointensity
- T2/FLAIR: cortical hyperintensity
- DWI/ADC: may show restriction due to cytotoxic oedema caused by the acute inflammatory lesions 4
- T1 C+ (Gd): cortical and adjacent leptomeninges may show enhancement
Treatment and prognosis
The disease is generally benign and self-limited, however some complications, as described above, can take the patient to a worse prognosis and lead to death.
In rare complicated cases a massive cerebellar oedema can require a surgical decompression of the posterior cranial fossa 4.
Differential diagnosis
Clinical features and the age group are essential when thinking of possible differential diagnoses. AC Acute cerebellitis limited to one cerebellar hemisphere may mimic a cerebellar tumour, especially:
- Lhermitte-Duclos disease
- medulloblastoma: atypical cerebellar location usually seen in adult patients
- cerebellar lymphoma: elderly patients
- paraneoplastic opsoclonus-myoclonus syndrome
-<p><strong>Acute cerebellitis (AC)</strong>, also known as <strong>acute cerebellar ataxia</strong>, is a rare inflammatory process characterised by a sudden onset of cerebellar dysfunction usually affecting children. It is related as a consequence of a primary or secondary infection, or much less commonly as a result of post-vaccinal reaction.</p><h4>Epidemiology</h4><p>Usually occurring in children under six years of age, AC is the most common cause of ataxia in the paediatric population. It is reported as a complication of several systemic infectious diseases, such as varicella infection (chickenpox) <sup>6</sup>. </p><p>Adult cases of cerebellitis are possible and well established in medical literature <sup>5</sup>. </p><h4>Clinical presentation</h4><p>A broad range of signs and symptoms may be present: fever, tremor, nystagmus, truncal ataxia, dysarthria, headache, nausea, vomiting and consciousness alterations. Signs of meningeal irritation and seizures may be observed less frequently <sup>1,4</sup>. </p><p>Some relevant complications have been described, such as:</p><ul>- +<p><strong>Acute cerebellitis</strong>, also known as <strong>acute cerebellar ataxia</strong>, is a rare inflammatory process characterised by a sudden onset of cerebellar dysfunction usually affecting children. It is related as a consequence of a primary or secondary infection, or much less commonly as a result of a post-vaccination reaction.</p><h4>Terminology</h4><p>The terms acute cerebellitis and acute cerebellar ataxia are often used interchangeably, as in this article, but they are considered separate by some authors <sup>9</sup>. Acute cerebellar ataxia is a milder form of acute cerebellitis or perhaps a mild subset of acute cerebellitis <sup>9</sup>. </p><h4>Epidemiology</h4><p>Usually occurring in children under six years of age, acute cerebellitis is the most common cause of ataxia in the paediatric population. It is reported as a complication of several systemic infectious diseases, such as varicella infection (chickenpox) <sup>6</sup>. </p><p>Adult cases of cerebellitis are possible and well established in medical literature <sup>5</sup>. </p><h4>Clinical presentation</h4><p>A broad range of signs and symptoms may be present: fever, tremor, nystagmus, truncal ataxia, dysarthria, headache, nausea, vomiting and consciousness alterations. Signs of meningeal irritation and seizures may be observed less frequently <sup>1,4</sup>. </p><p>Some relevant complications have been described, such as:</p><ul>
-</ul><h6>Laboratory findings</h6><ul><li>CSF pleocytosis <sup>4</sup> </li></ul><h4>Pathology</h4><p>AC has been associated with a large number of infectious agents, such as: coxsackievirus, echovirus, enteroviruses, <a title="EBV encephalitis" href="/articles/epstein-barr-virus-encephalitis">Epstein-Barr virus</a>, hepatitis A, herpes simplex virus I, human herpesvirus 6, measles, rubella, <a href="/articles/mumps">mumps</a>, parvovirus B19, <em>Borrelia burgdorferi</em> (Lyme disease), <a href="/articles/cerebral-malaria-2">malaria</a>, <em>Mycoplasma pneumoniae</em>, and typhoid fever <sup>2,4,6</sup>.</p><p>Acute cerebellar ataxia following vaccination for varicella, hepatitis B, and rabies has been reported <sup>6-8</sup>. </p><h4>Radiographic features</h4><h5>CT</h5><p>Cerebellar images can be normal due the CT limitations on the evaluation of posterior fossa. Nonetheless, complications like compression of the brain stem and obstructive hydrocephalus, when present, are identified on CT images and may guide for further investigation. </p><h5>MRI </h5><p>Usually the cerebellar hemispheres are symmetric. It may show a homogeneous mass effect due the cerebellar swelling <sup>1,4</sup>. </p><ul>- +</ul><h6>Laboratory findings</h6><ul><li>CSF pleocytosis <sup>4</sup> </li></ul><h4>Pathology</h4><p>Acute cerebellitis has been associated with a large number of infectious agents, such as: coxsackievirus, echovirus, enteroviruses, <a href="/articles/epstein-barr-virus-encephalitis-2">Epstein-Barr virus</a>, hepatitis A, herpes simplex virus I, human herpesvirus 6, measles, rubella, <a href="/articles/mumps">mumps</a>, parvovirus B19, <em>Borrelia burgdorferi</em> (Lyme disease), <a href="/articles/cerebral-malaria-2">malaria</a>, <em>Mycoplasma pneumoniae</em>, and typhoid fever <sup>2,4,6</sup>.</p><p>Acute cerebellar ataxia following vaccination for varicella, hepatitis B, and rabies has been reported <sup>6-8</sup>. </p><h4>Radiographic features</h4><h5>CT</h5><p>Cerebellar images can be normal due the CT limitations on the evaluation of posterior fossa. Nonetheless, complications like compression of the brain stem and obstructive hydrocephalus, when present, are identified on CT images and may guide for further investigation. </p><h5>MRI </h5><p>Usually, the cerebellar hemispheres are symmetric. It may show a homogeneous mass effect due the cerebellar swelling <sup>1,4</sup>. </p><ul>
-</ul><h4>Treatment and prognosis</h4><p>The disease is generally benign and self-limited, however some complications, as described above, can take the patient to a worse prognosis and lead to death. </p><p>In rare complicated cases a massive cerebellar oedema can require a surgical decompression of the posterior cranial fossa <sup>4</sup>.</p><h4>Differential diagnosis</h4><p>Clinical features and the age group are essential when thinking of possible differential diagnoses. AC limited to one cerebellar hemisphere may mimic a cerebellar tumour, especially:</p><ul>- +</ul><h4>Treatment and prognosis</h4><p>The disease is generally benign and self-limited, however some complications, as described above, can take the patient to a worse prognosis and lead to death. </p><p>In rare complicated cases a massive cerebellar oedema can require a surgical decompression of the posterior cranial fossa <sup>4</sup>.</p><h4>Differential diagnosis</h4><p>Clinical features and the age group are essential when thinking of possible differential diagnoses. Acute cerebellitis limited to one cerebellar hemisphere may mimic a cerebellar tumour, especially:</p><ul>
- +<li><a title="paraneoplastic opsoclonus-myoclonus syndrome" href="/articles/paraneoplastic-opsoclonus-myoclonus-syndrome">paraneoplastic opsoclonus-myoclonus syndrome</a></li>
References changed:
- 9. Desai J, Mitchell WG. Acute cerebellar ataxia, acute cerebellitis, and opsoclonus-myoclonus syndrome. (2012) Journal of child neurology. 27 (11): 1482-8. <a href="https://doi.org/10.1177/0883073812450318">doi:10.1177/0883073812450318</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/22805251">Pubmed</a> <span class="ref_v4"></span>
Image ( destroy )
Image ( destroy )
Image 1 MRI (T2) ( update )





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.