
Benign notochordal cell tumor
Updates to Article Attributes
Benign notochordal cell tumour (BNCT) is an asymptomatic vertebral lesion that is usually asymptomatic and discovered incidentally on imaging of the head or spine. As this is a poorly recognised entity, it can often be confused with aggressive vertebral lesions, such as a chordoma, when it is seen on imaging.
Epidemiology
Autopsy studies show BNCTs are extremely common with a reported incidence of up to 20% in cadaveric specimens 1. While only the larger of these lesions can be seen on imaging it is felt they are under reported 2.
Clinical presentation
The vast majority of lesions are asymptomatic but a small proportion of patients can present with chronic back pain and coccydynia 2.
Pathology
Location
The distribution is similar to chordomas:
- clivus (50%)
- vertebrae
- sacrum/coccyx
Radiographic features
CT
-
vertebral body sclerosis
- can extend to cortex or involve entire vertebrae
- preserved trabeculae
- no cortical destruction
MRI
-
well defined osseous lesions
- T1: low or isointense
- T2: hyperintense
- T1 C+ (Gd): no enhancement
- DWI: no restricted diffusion
- no soft tissue component
Nuclear medicine
Often show no uptake on bone scintigraphy.
Treatment and prognosis
While there is a consensus that no specific treatment is required for asymptomatic lesions, the long term malignant potential of BNCTs to transform into chordomas is not known and many advocate interval follow up 5.
Differential diagnosis
- chordoma
- ecchordosis physaliphora
- notochordal vestiges of the intervertebral disk
-<p><strong>Benign notochordal cell tumour (BNCT) </strong>is an asymptomatic lesion that is usually asymptomatic and discovered incidentally on imaging of the head or spine. As this is a poorly recognised entity, it can often be confused with aggressive vertebral lesions, such as a <a title="Chordoma" href="/articles/chordoma">chordoma</a>, when it is seen on imaging.</p><h4>Epidemiology</h4><p>Autopsy studies show BNCTs are extremely common with a reported incidence of up to 20% in cadaveric specimens <sup>1</sup>. While only the larger of these lesions can be seen on imaging it is felt they are under reported <sup>2</sup>.</p><p>Clinical presentation</p><p> </p><h4>Pathology</h4><h4> </h4><h4>Radiographic features</h4><p> </p><h4>Differential diagnosis</h4><ul>-<li><a title="Chordoma" href="/articles/chordoma">chordoma</a></li>-<li><a title="Ecchordosis physaliphora" href="/articles/ecchordosis-physaliphora">ecchordosis physaliphora</a></li>- +<p><strong>Benign notochordal cell tumour (BNCT) </strong>is an asymptomatic vertebral lesion that is usually asymptomatic and discovered incidentally on imaging of the head or spine. As this is a poorly recognised entity, it can often be confused with aggressive vertebral lesions, such as a <a href="/articles/chordoma">chordoma</a>, when it is seen on imaging.</p><h4>Epidemiology</h4><p>Autopsy studies show BNCTs are extremely common with a reported incidence of up to 20% in cadaveric specimens <sup>1</sup>. While only the larger of these lesions can be seen on imaging it is felt they are under reported <sup>2</sup>.</p><h4>Clinical presentation</h4><p>The vast majority of lesions are asymptomatic but a small proportion of patients can present with chronic back pain and coccydynia <sup>2</sup>.</p><h4>Pathology</h4><h5>Location</h5><p>The distribution is similar to chordomas:</p><ul>
- +<li>clivus (50%)</li>
- +<li>vertebrae</li>
- +<li>sacrum/coccyx</li>
- +</ul><h4>Radiographic features</h4><h5>CT</h5><ul>
- +<li>vertebral body sclerosis<ul><li>can extend to cortex or involve entire vertebrae</li></ul>
- +</li>
- +<li>preserved trabeculae</li>
- +<li>no cortical destruction</li>
- +</ul><h5>MRI</h5><ul>
- +<li>well defined osseous lesions<ul>
- +<li>
- +<strong>T1</strong>: low or isointense</li>
- +<li>
- +<strong>T2</strong>: hyperintense</li>
- +<li>
- +<strong>T1 C+ (Gd): </strong>no enhancement</li>
- +<li>
- +<strong>DWI</strong>: no restricted diffusion</li>
- +</ul>
- +</li>
- +<li>no soft tissue component</li>
- +</ul><h5>Nuclear medicine</h5><p>Often show no uptake on bone scintigraphy.</p><h4>Treatment and prognosis</h4><p>While there is a consensus that no specific treatment is required for asymptomatic lesions, the long term malignant potential of BNCTs to transform into chordomas is not known and many advocate interval follow up <sup>5</sup>.</p><h4>Differential diagnosis</h4><ul>
- +<li><a href="/articles/chordoma">chordoma</a></li>
- +<li><a href="/articles/ecchordosis-physaliphora">ecchordosis physaliphora</a></li>
References changed:
- 1. Yamaguchi T, Suzuki S, Ishiiwa H, Shimizu K, Ueda Y. Benign notochordal cell tumors: A comparative histological study of benign notochordal cell tumors, classic chordomas, and notochordal vestiges of fetal intervertebral discs. (2004) The American journal of surgical pathology. 28 (6): 756-61. <a href="https://www.ncbi.nlm.nih.gov/pubmed/15166667">Pubmed</a> <span class="ref_v4"></span>
- 2. Amer HZ, Hameed M. Intraosseous benign notochordal cell tumor. (2010) Archives of pathology & laboratory medicine. 134 (2): 283-8. <a href="https://doi.org/10.1043/1543-2165-134.2.283">doi:10.1043/1543-2165-134.2.283</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/20121620">Pubmed</a> <span class="ref_v4"></span>
- 3. Nishiguchi T, Mochizuki K, Ohsawa M, Inoue T, Kageyama K, Suzuki A, Takami T, Miki Y. Differentiating benign notochordal cell tumors from chordomas: radiographic features on MRI, CT, and tomography. (2011) AJR. American journal of roentgenology. 196 (3): 644-50. <a href="https://doi.org/10.2214/AJR.10.4460">doi:10.2214/AJR.10.4460</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/21343509">Pubmed</a> <span class="ref_v4"></span>
- 3. Nishiguchi T, Mochizuki K, Ohsawa M, Inoue T, Kageyama K, Suzuki A, Takami T, Miki Y. Differentiating benign notochordal cell tumors from chordomas: radiographic features on MRI, CT, and tomography. (2011) AJR. American journal of roentgenology. 196 (3): 644-50. <a href="https://doi.org/10.2214/AJR.10.4460">doi:10.2214/AJR.10.4460</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/21343509">Pubmed</a> <span class="ref_v4"></span>
- 4. Nouh MR, Eid AF. Magnetic resonance imaging of the spinal marrow: Basic understanding of the normal marrow pattern and its variant. (2015) World journal of radiology. 7 (12): 448-58. <a href="https://doi.org/10.4329/wjr.v7.i12.448">doi:10.4329/wjr.v7.i12.448</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/26753060">Pubmed</a> <span class="ref_v4"></span>
- 4. Yamaguchi T, Yamato M, Saotome K. First histologically confirmed case of a classic chordoma arising in a precursor benign notochordal lesion: differential diagnosis of benign and malignant notochordal lesions. (2002) Skeletal radiology. 31 (7): 413-8. <a href="https://doi.org/10.1007/s00256-002-0514-z">doi:10.1007/s00256-002-0514-z</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/12107574">Pubmed</a> <span class="ref_v4"></span>
- 4. Yamaguchi T, Yamato M, Saotome K. First histologically confirmed case of a classic chordoma arising in a precursor benign notochordal lesion: differential diagnosis of benign and malignant notochordal lesions. (2002) Skeletal radiology. 31 (7): 413-8. <a href="https://doi.org/10.1007/s00256-002-0514-z">doi:10.1007/s00256-002-0514-z</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/12107574">Pubmed</a> <span class="ref_v4"></span>
Tags changed:
- cases
Systems changed:
- Musculoskeletal
- Central Nervous System
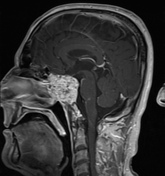
Image 1 MRI (T1 C+) ( create )





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.