
Laryngeal trauma
Updates to Article Attributes
Laryngeal trauma is uncommon in the setting of external blunt or penetrating trauma. The larynx may also be injured internally, for example during endotracheal intubation.
Clinical presentation
Symptoms include hoarseness, larygneal pain, dyspnoea, and/or dysphagia. Also stridor, haemoptysis, subcutaneous emphysema and tenderness/deformity of the larynx skeleton may be present.
Pathology
The following laryngeal structures may injured in isolation or combination 1,2
- laryngeal oedema, haematoma and/or mucosal lacerations
- thyroid and/or cricoid cartilage fracture
- laryngeal rupture
- cricotracheal separation
- cervical tracheal injury
The hyoid bone, although technically not part of the larynx, can also be fractured.
Mechanism
The larynx may be injured in a number of ways 1,2:
- external blunt: motor vehicle accidents, "clothesline" accidents, strangulation, falls, sporting injuries
- external penetrating: stabbing, shooting
- internal blunt: iatrogenic during endotracheal intubation or fibroendoscopic examination
Associations
Other injuries are common 1:
- base of skull or facial fractures (~20%)
- cervical spine fractures (~10%)
- thoracic and abdominal injuries
Radiographic features
CT is the modality of choice. Review of airway obstruction includes evaluation of oedema, haematoma, foreign body or displaced fractures.
CT review for larynx function should also include close inspection for lacerations especially to the vocal cord and anterior commisure, and arytenoid cartilage dislocation or avulsion.
Treatment and prognosis
The key goals of management are:
- maintaining airway: preserve life
- restoring function to larynx: voice quality
Practical points
- Patients who are uncooperative or unstable and may not be in the normal anatomical position on the CT scanner. Often useful to use a 3D workstation to facilitate proper review of soft tissue injuries to the true cord versus false cord, and position of the cricoid cartilages.
-
CT is advantageous over laryngoscopy and clinical exam for:
- detection of cartilage fractures
- evaluation of the subglottic and anterior commissure regions which are poorly visualized on endoscopy
- Do not forget to assess for associated cervical spine and vascular injuries.
- A key indirect sign of laryngeal injury is subcutaneous emphysema. If this is present look for subtle laryngeal and tracheal injury. There can be a ball-valve derangement that forces massive amounts of air into the neck and chest leading to tracheal displacement and pneumothorax. Thus, patients with laryngeal trauma should not have excessive mask ventilation.
- Look for tracheolaryngeal separation: should not have intubation, but require tracheostomy.
-<p><strong>Laryngeal trauma </strong>is uncommon in the setting of external blunt or penetrating trauma. The <a title="Larynx" href="/articles/larynx">larynx</a> may also be injured internally, for example during endotracheal intubation. </p><h4>Pathology</h4><p>The following laryngeal structures may injured in isolation or combination <sup>1,2</sup></p><ul>- +<p><strong>Laryngeal trauma </strong>is uncommon in the setting of external blunt or penetrating trauma. The <a href="/articles/larynx">larynx</a> may also be injured internally, for example during endotracheal intubation.</p><h4>Clinical presentation</h4><p>Symptoms include hoarseness, larygneal pain, dyspnoea, and/or <a href="/articles/dysphagia">dysphagia</a>. Also stridor, haemoptysis, <a href="/articles/subcutaneous-emphysema">subcutaneous emphysema</a> and tenderness/deformity of the larynx skeleton may be present. </p><h4>Pathology</h4><p>The following laryngeal structures may injured in isolation or combination <sup>1,2</sup></p><ul>
-<a title="thyroid cartilage" href="/articles/thyroid-cartilage">thyroid</a> and/or <a title="cricoid cartilage" href="/articles/cricoid-cartilage">cricoid cartilage</a> fracture</li>- +<a href="/articles/thyroid-cartilage-1">thyroid</a> and/or <a href="/articles/cricoid-cartilage">cricoid cartilage</a> fracture</li>
-</ul><p>The <a title="Hyoid bone" href="/articles/hyoid-bone">hyoid bone</a>, although technically not part of the larynx, can also be fractured. </p><h5>Mechanism</h5><p>The larynx may be injured in a number of ways <sup>1,2</sup>:</p><ul>- +</ul><p>The <a href="/articles/hyoid-bone">hyoid bone</a>, although technically not part of the larynx, can also be fractured.</p><h5>Mechanism</h5><p>The larynx may be injured in a number of ways <sup>1,2</sup>:</p><ul>
-<li>base of skull or <a title="Facial fractures" href="/articles/facial-fractures">facial fractures</a> (~20%)</li>- +<li>base of skull or <a href="/articles/facial-fractures">facial fractures</a> (~20%)</li>
-<a title="Cervical spine fractures" href="/articles/cervical-spine-fractures">cervical spine fractures</a> (~10%)</li>- +<a href="/articles/cervical-spine-fractures">cervical spine fractures</a> (~10%)</li>
-</ul>- +</ul><h4>Radiographic features</h4><p>CT is the modality of choice. Review of airway obstruction includes evaluation of oedema, haematoma, foreign body or displaced fractures.</p><p>CT review for larynx function should also include close inspection for lacerations especially to the <a href="/articles/vocal-cord">vocal cord</a> and anterior commisure, and <a href="/articles/arytenoid-cartilage">arytenoid cartilage</a> dislocation or avulsion.</p><h4>Treatment and prognosis</h4><p>The key goals of management are:</p><ul>
- +<li>maintaining airway: preserve life</li>
- +<li>restoring function to larynx: voice quality</li>
- +</ul><h4>Practical points</h4><ol>
- +<li>Patients who are uncooperative or unstable and may not be in the normal anatomical position on the CT scanner. Often useful to use a 3D workstation to facilitate proper review of soft tissue injuries to the true cord versus false cord, and position of the cricoid cartilages. </li>
- +<li>CT is advantageous over laryngoscopy and clinical exam for:<ul>
- +<li>detection of cartilage fractures</li>
- +<li>evaluation of the subglottic and anterior commissure regions which are poorly visualized on endoscopy</li>
- +</ul>
- +</li>
- +<li>Do not forget to assess for associated cervical spine and vascular injuries.</li>
- +<li>A key indirect sign of laryngeal injury is subcutaneous emphysema. If this is present look for subtle laryngeal and tracheal injury. There can be a ball-valve derangement that forces massive amounts of air into the neck and chest leading to tracheal displacement and <a href="/articles/pneumothorax">pneumothorax</a>. Thus, patients with laryngeal trauma should not have excessive mask ventilation.</li>
- +<li>Look for tracheolaryngeal separation: should not have intubation, but require tracheostomy.</li>
- +</ol>
References changed:
- 2. Mancuso AA, Hanafee WN. Computed tomography of the injured larynx. Radiology. 1979;133 (1): 139-44. <a href="http://dx.doi.org/10.1148/133.1.139">doi:10.1148/133.1.139</a> - <a href="http://www.ncbi.nlm.nih.gov/pubmed/472282">Pubmed citation</a><span class="auto"></span>
- 1. Becker M, Leuchter I, Platon A et-al. Imaging of laryngeal trauma. Eur J Radiol. 2014;83 (1): 142-54. <a href="http://dx.doi.org/10.1016/j.ejrad.2013.10.021">doi:10.1016/j.ejrad.2013.10.021</a> - <a href="http://www.ncbi.nlm.nih.gov/pubmed/24238937">Pubmed citation</a><span class="auto"></span>
- 3. Offiah C, Hall E. Imaging assessment of penetrating injury of the neck and face. Insights Imaging. 2012;3 (5): 419-31. <a href="http://dx.doi.org/10.1007/s13244-012-0191-y">doi:10.1007/s13244-012-0191-y</a> - <a href="http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3443277">Free text at pubmed</a> - <a href="http://www.ncbi.nlm.nih.gov/pubmed/22945428">Pubmed citation</a><span class="auto"></span>
- 4. Francis S, Gaspard DJ, Rogers N et-al. Diagnosis and management of laryngotracheal trauma. J Natl Med Assoc. 2002;94 (1): 21-4. <a href="http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2594079">Free text at pubmed</a> - <a href="http://www.ncbi.nlm.nih.gov/pubmed/11837348">Pubmed citation</a><span class="auto"></span>
- 5. Johnson J. Bailey's Head and Neck Surgery: Otolaryngology (2 volume set). LWW. ISBN:1609136020. <a href="http://books.google.com/books?vid=ISBN1609136020">Read it at Google Books</a> - <a href="http://www.amazon.com/gp/product/1609136020">Find it at Amazon</a><span class="auto"></span>
Systems changed:
- Head & Neck
Image 1 CT (C+ arterial phase) ( create )

Image 2 CT (non-contrast) ( create )

Image 3 CT (bone window) ( create )
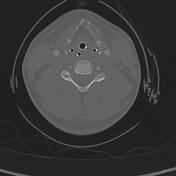
Image 4 CT (bone window) ( create )

Image 5 Annotated image (Axial non-contrast CT) ( create )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.